| PARI Sprint Star – (with red insert) |  | Total Output Rate: 450 mg/min MMD(mass median diameter):2.2µm Mass percentage below 5µm: 89% | When used with Pari SX compressor. Fine particle size for targeted delivery to the peripheral regions of the lung. |
| PARI Sprint – (with blue insert) |  | Total Output Rate: 590 mg/min MMD(mass median diameter):2.9µm Mass percentage below 5µm:75% | When used with Pari SX compressor. |
| InnoSpire Deluxe compressor |  | MMAD – 3.4 µm Fine particle fraction – 67% below 5µm Weight – 2.2kg | To be used with the SideStream Re-usable or SideStream Plus nebulisers. |
| PARI Boy Classic compressor |  | Warranty: four (4) years Power supply: 230V~ 50/60Hz – 0,7 A – 80 W Dimensions: W 19,2 x H 14,5 x D 15 cm Weight: 1.7 kg | Replace filter every year. Service when pressures significantly fall below 1.5 bar. |
| PARI Sinus (compressor can also be used with Pari Sprint and Sprint Star) |  | Total Output Rate: 220 mg/min MMD(mass median diameter):3.2µm Mass percentage below 5µm: 71% | Pulsed aerosol delivery to the nasal cavities |
| Bird e-Chamber |  | MMAD of 2.5µm – 4.5µm Nebuliser rate of 0.3ml/min – 0.7ml/min | Portable light weight nebuliser. Only suitable for nebulised saline and hypertonic saline. |
| PARI eFlow | 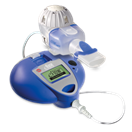 | Total Output Rate: 500 mg/min MMD(mass median diameter):4.1µm Mass percentage below 5µm: 64% See Technipro Pulmomed video for use and care of this device: http://www.pulmomed.com.au/eFlowrapidvideo.html | Max fill volume – 6mls Weight – 300gms |
| Flaem NebulAir+ compressor |  | MMAD: 2.21µm Fine particle fraction: 84.2% below 5 µm Weight: 2.4 kg Warranty: 3 years Made in Italy | When used with Flaem RF7+ nebuliser Heavy duty compressor for continuous use Capable of producing up to 14 L/min of flow |
| Flaem RF7+ nebuliser |  | MMAD: 2.21µm Fine particle fraction: 84.2% below 5 µm Can be used with any nebuliser compressor Dual speed valve to select between faster treatment or maximum drug delivery | When used with Flaem NebulAir+ compressor |
| Flaem RespirAir compressor |  | MMAD: 2.53µm Fine particle fraction: 79.6% below 5 µm Weight: 1.45 kg Warranty: 3 years Made in Italy | When used with Flaem RF7+ nebuliser Compact, sleek and powerful with high quality ABS polymer finish capable of producing up to 10 L/min flow |



")