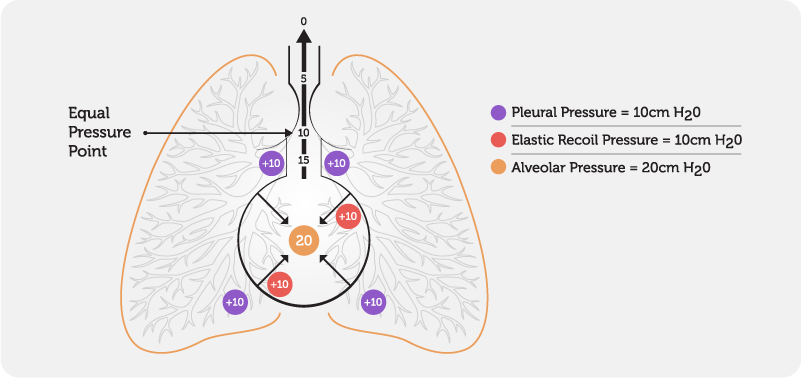
Physiology – The rationale behind a huff is based on the equal pressure point (EPP) – the point at which pressure within the bronchi equals peri-bronchial pressure (outside the airway). (Fig. 4).
Fig. 4 Equal Pressure Point
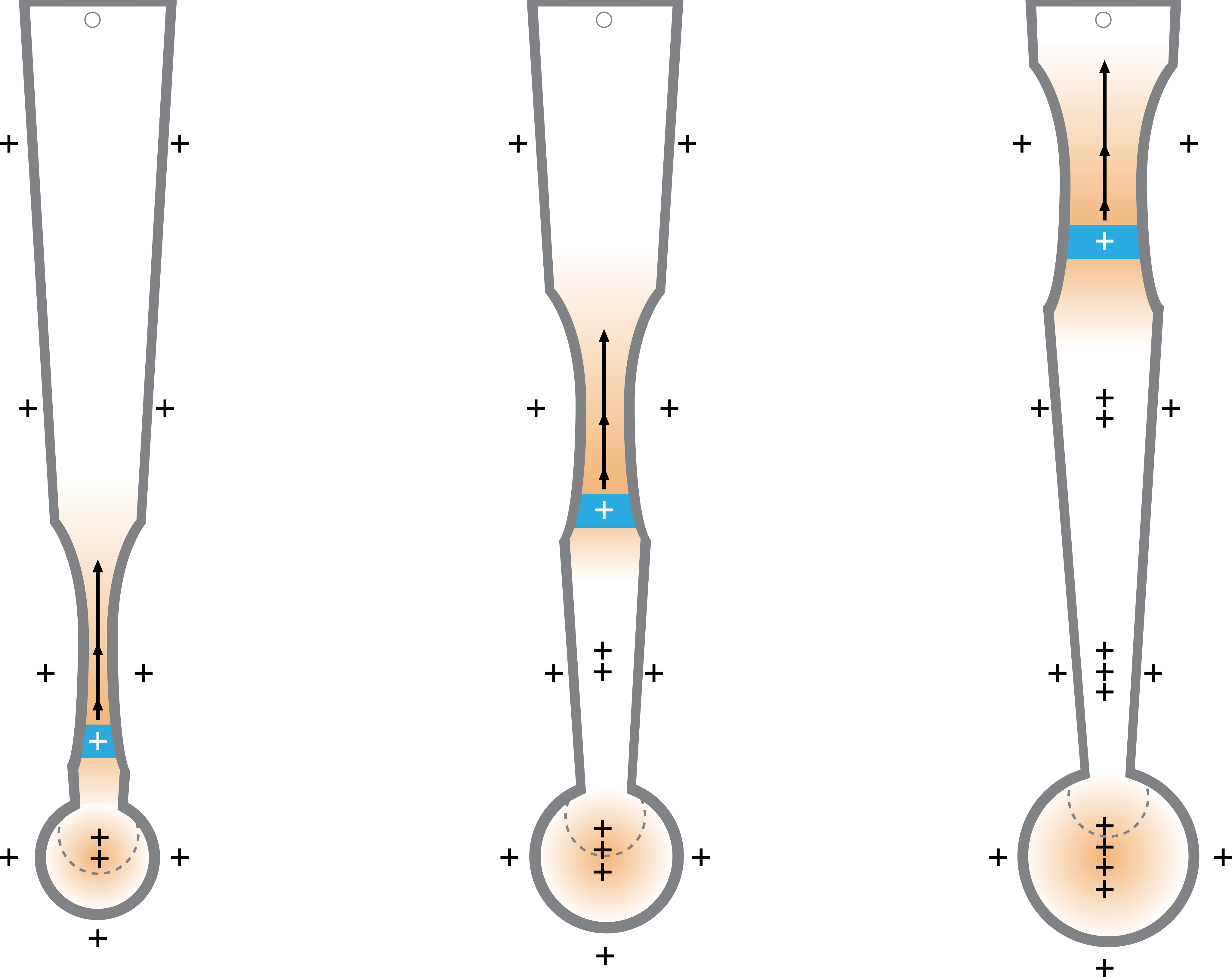
During normal respiration, the EPP occurs in airways protected by cartilaginous rings which help to prevent airway collapse. During a forced expiration, the pressure outside the airway remains relatively constant, whilst the pressure inside the airway decreases from the peripheral airways to the mouth, resulting in airway compression. With a forced expiration, a wave of EPP’s move peripherally into smaller airways as the lung volume decreases and the pressure within the airway falls. This, together with the turbulent airflow created, facilitates the movement of secretions downstream towards the mouth. The position of the EPP is dependent on lung volume and the pressure outside the airway(Fig 5)
Fig. 5 Movement of the Equal Pressure Point
Key: Blue segment = equal pressure point, Plus signs = pressure within and outside the lung, Black arrows = airflow