Physiology – Large inspiratory volumes are believed to facilitate collateral ventilation . This can be further enhanced by a breath hold. (Menkes & Traystman 1997). Resistance to airflow within the canals of Martin, channels of Lambert and Pores of Kohn, (between the bronchioles and alveoli), is usually high, with little movement during tidal volume breaths. With increasing inspired volumes, the resistance decreases and air flows through these channels to enhance expiratory flow behind the secretions (see Fig 3).
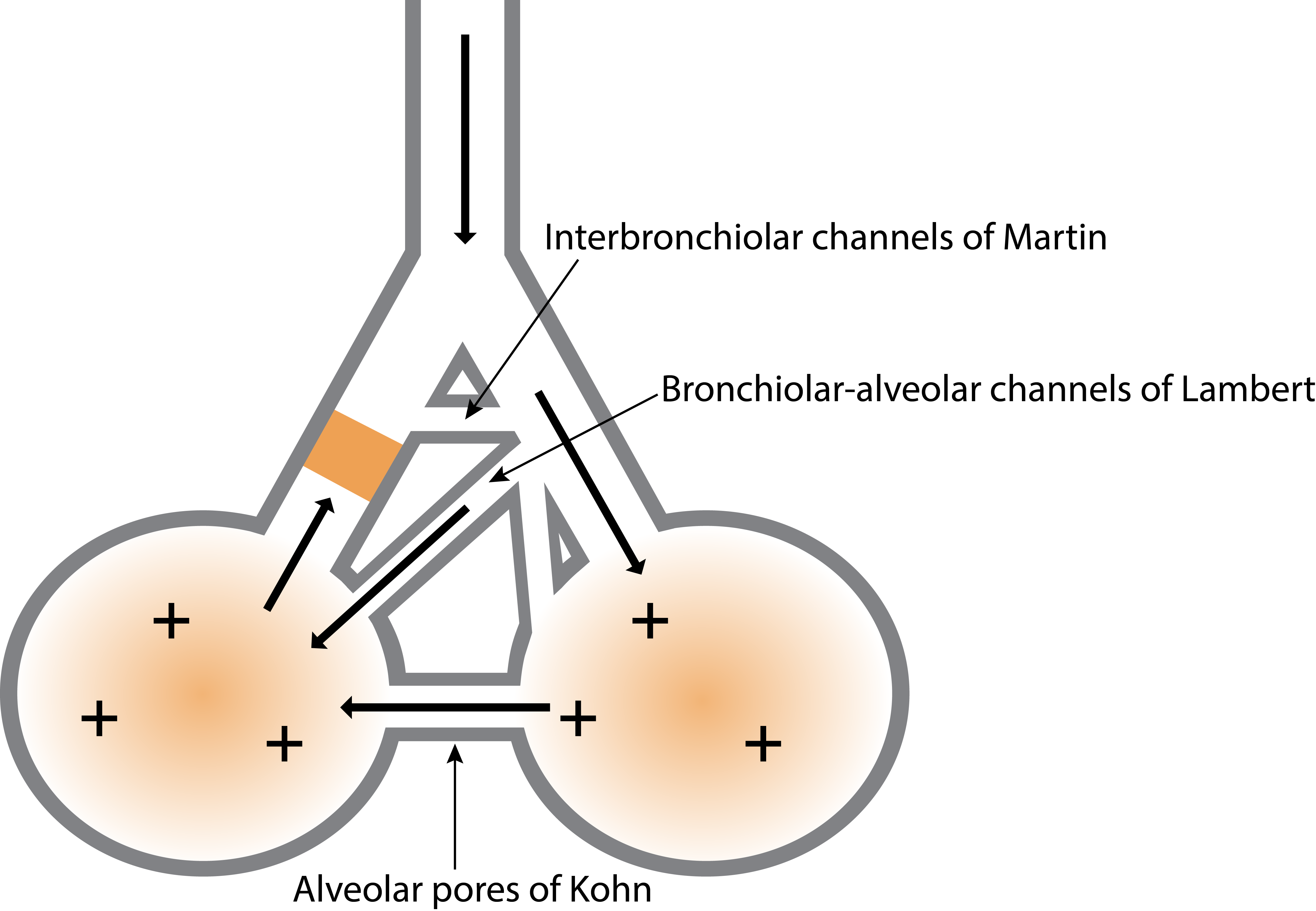
Fig. 3 Collateral Ventilation Channels.
Key – Arrows – movement of air flow, + signs – air pressure, yellow block – sputum plug
At high lung volumes, achieved during thoracic expansion exercises, the expanding forces between alveoli are greater than at tidal volume and may assist with the re-expansion of lung tissue. This is known as alveolar inter-dependence (Fig. 4). During inspiration, the expanding alveoli exert forces on the adjacent alveoli which enhance the recruitment of lung units.
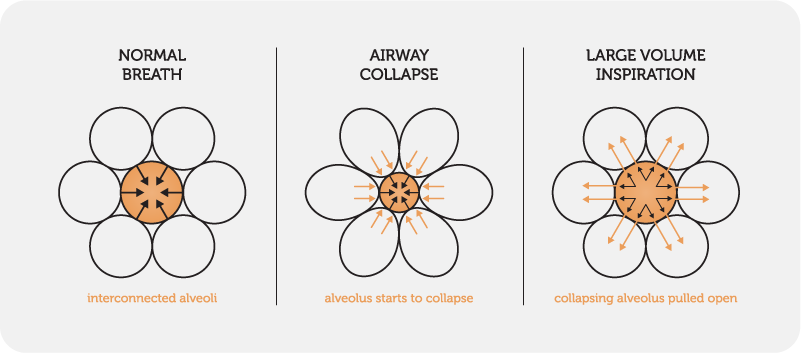 Fig. 4 Interdependence of alveoli
Fig. 4 Interdependence of alveoli

Physiology – The rationale behind a huff is based on the equal pressure point (EPP) – the point at which pressure within the bronchi equals peri-bronchial pressure (outside the airway). (Fig. 6).
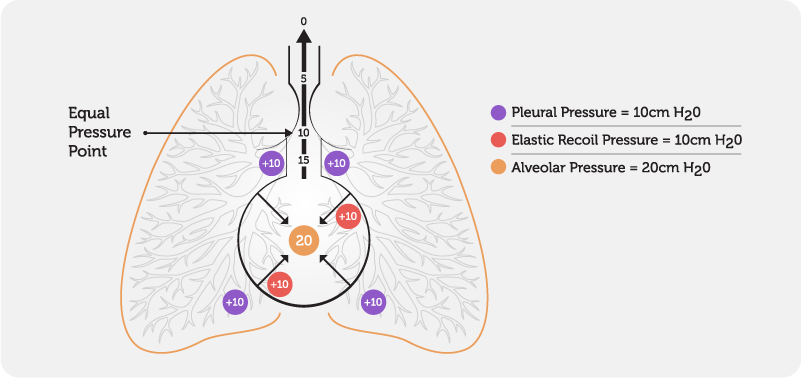
Fig. 6 Equal Pressure Point
During normal respiration, the EPP occurs in airways protected by cartilaginous rings which help to prevent airway collapse.
During a forced expiration, the pressure outside the airway remains relatively constant, whilst the pressure inside the airway decreases from the peripheral airways to the mouth, resulting in airway compression.
With a forced expiration, a wave of EPP’s move peripherally into smaller airways as the lung volume decreases and the pressure within the airway falls. This, together with the turbulent airflow created, facilitates the movement of secretions downstream towards the mouth. The position of the EPP is dependent on lung volume and the pressure outside the airway. (Fig 7.)The EPP moves upstream towards the alveoli when the volume inside the lungs decreases and/or the pressure outside the airway increases. The EPP moves downstream towards the mouth when the volume inside the lungs increases and/or the pressure outside the airway decreases. Therefore, to move secretions from peripheral airways, it is more effective to commence huffing at low lung volumes and to progress to medium and finally large lung volumes.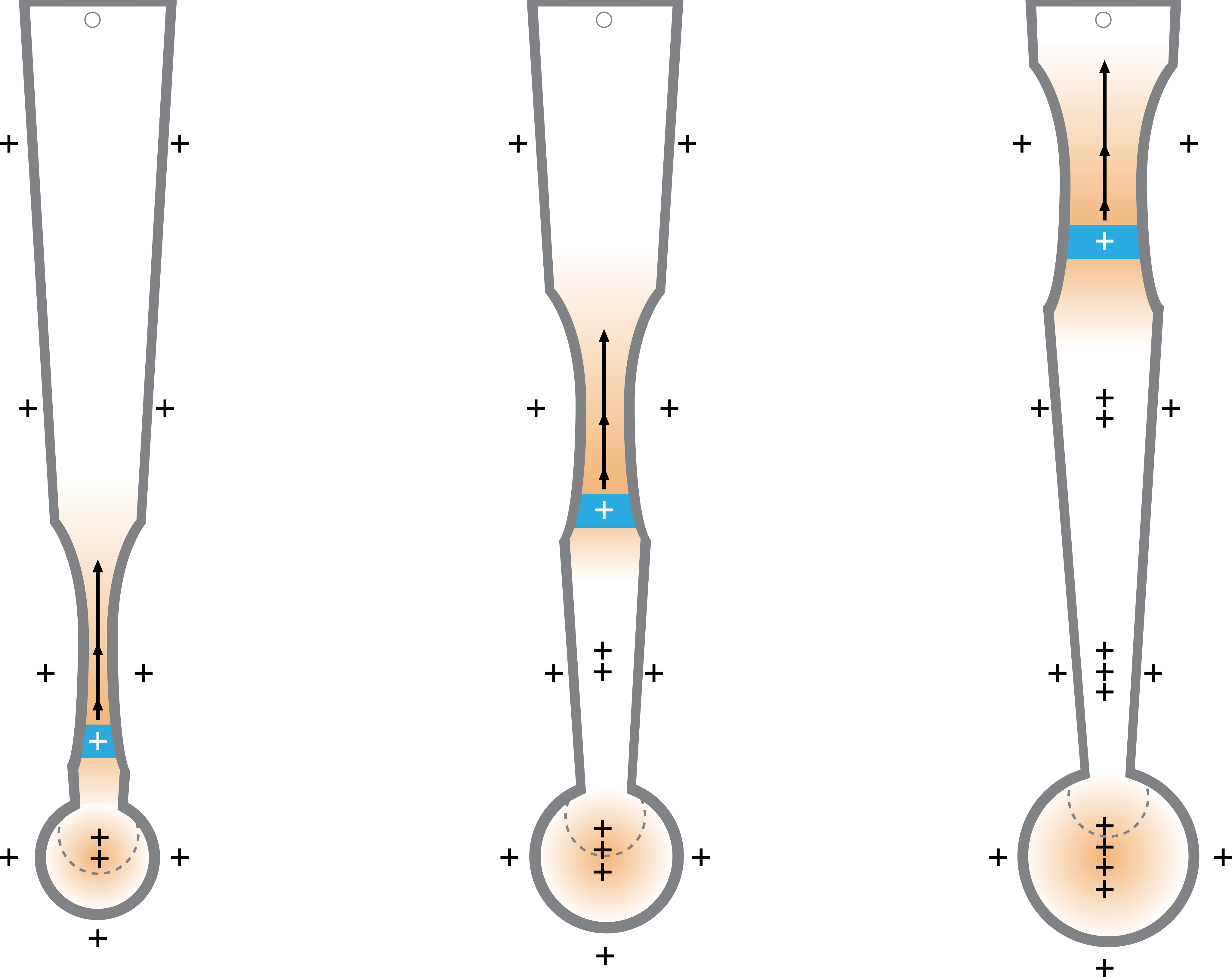
Fig. 7 Movement of the Equal Pressure Point.
Key: Blue segment – equal pressure point, + sign(s) – pressure within and outside the airway, arrows – airflow