Bronchiectasis is defined as irreversible dilatation of a portion of the bronchial tree. The three most important mechanisms that contribute to the pathogenesis of bronchiectasis are infection, airway obstruction and peribronchial fibrosis.
Imaging plays a pivotal role in the diagnosis of bronchiectasis. High-resolution computed tomography (HRCT) is the cornerstone in the radiological diagnosis of clinically suspicious cases. HRCT is the most sensitive and specific non-invasive method for diagnosing bronchiectasis. In addition to making the diagnosis, the pattern of disease on HRCT may enable one to limit the differential to a single/few specific causative entities.
The CXR in affected individuals is often normal or shows non specific findings. Its role has largely been reduced to surveillance for intercurrent infection, progressive lobar collapse or suspected development of cavitary disease in patients with known bronchiectasis.
Certain descriptive terms have been used in reporting of bronchiectasis. These only describe the appearance of the involved airways but do not elude to a specific cause.
These terms include:
Cylindrical (tram track sign):
This description applies to dilated airways seen in a horizontal orientation.
Signet-ring:
This describes airways viewed in a transverse plane. The dilated airway lies adjacent to a pulmonary artery branch giving the appearance of a ring
Varicose
Implies non uniform bronchial dilatation.
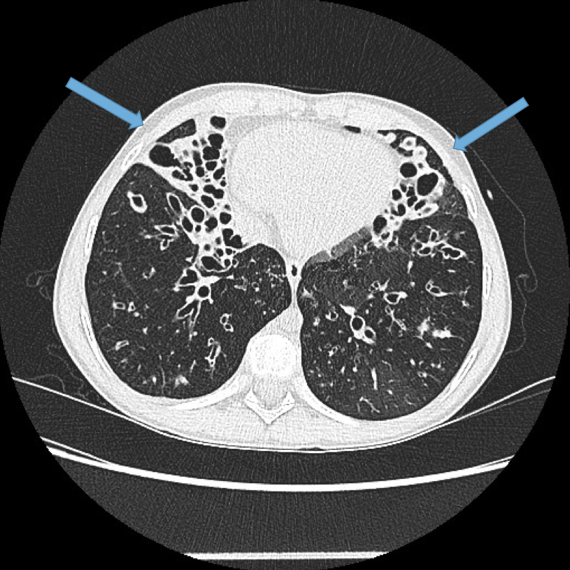
Cystic or saccular
A cluster of thin walled cystic spaces
CXR findings
Direct signs
Parallel line opacities (tram tracking) Fig 1a, b
Tubular opacities (mucous filled bronchi) Fig 2
Ring opacities (dilated end-on bronchi) Fig 1
Indirect signs
Lobar atelectasis (secondary to mucous plugging) Fig 1
Compensatory overinflation of the less affected lobe/lung Fig 1
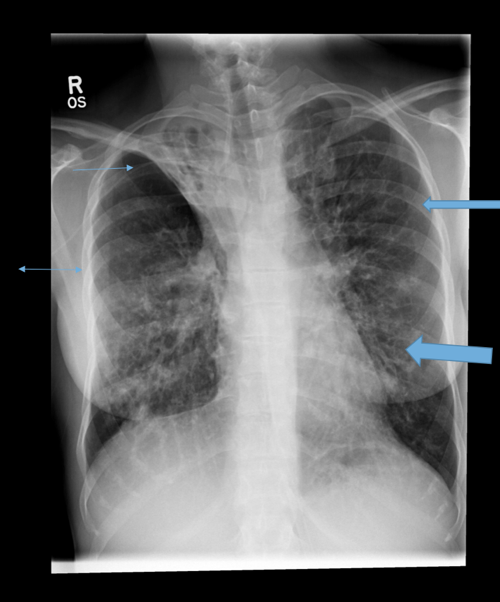
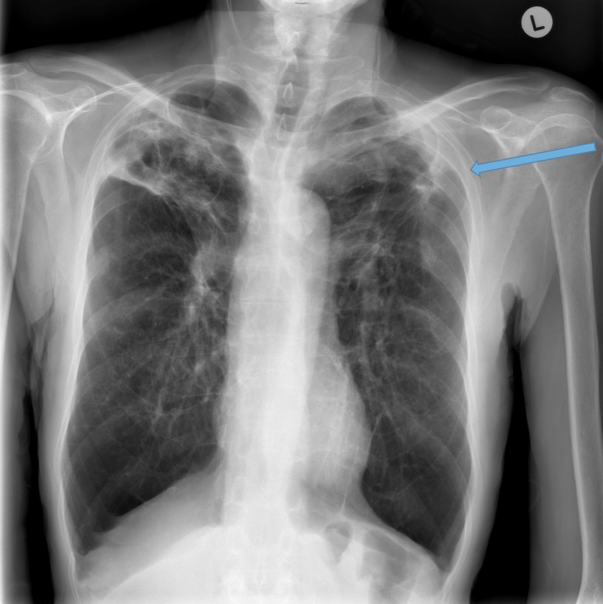
Fig 1a. Young adult with cystic fibrosis. Thin arrow: right upper lobe collapse. Thick arrow: ring shadow. Fat arrow: tram tracking. Double arrow: compensatory hyperinflation
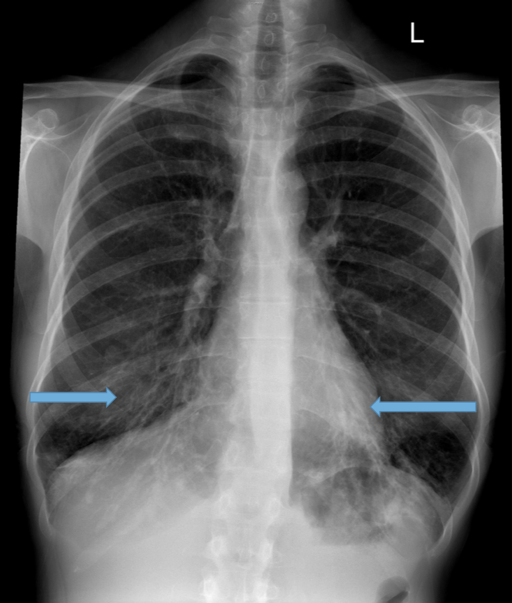
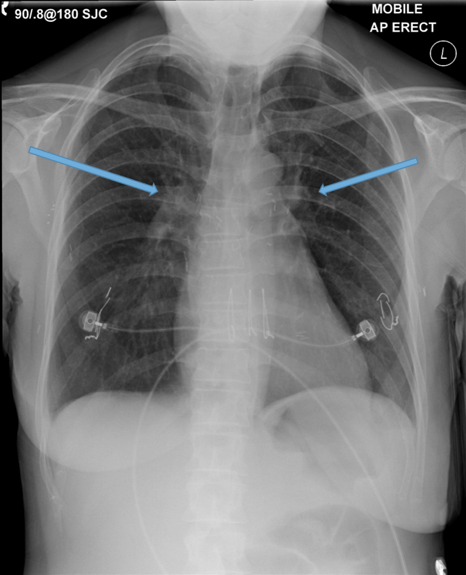
Fig 1b. Elderly man with COPD and bronchiectasis. Arrows: tram tracking appearance of dilated lower lobe bronchi
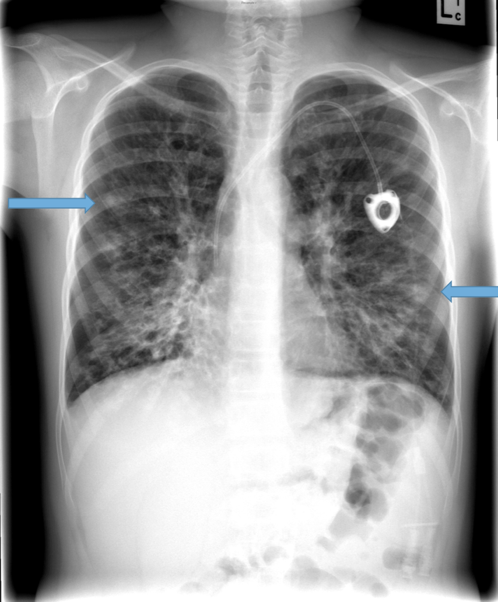
Fig 2. Young adult with cystic fibrosis. Arrows demonstrate mucous plugging of dilated airways.
Multidetector CT Imaging Technique
Multidetector CT scanners enable volumetric data acquisition with scans obtained through the entire thorax in a single breath-hold. This can be obtained in a few seconds or less thereby minimising respiratory and cardiac motion artefact. Images can then be reconstructed in multiple planes and slice thicknesses. It is recommended that thin slice images be reconstructed ≤ 1mm every 10mm, i.e. non contiguous scans. With this technique there are gaps in the viewed images therefore a second series should also be provided from the volumetric dataset containing thicker (3mm) but contiguous slices. This ensures that additional pathologies such as small lung nodules or neoplasms are not inadvertently missed.
Occasionally it may be helpful to also acquire expiratory images to assess the degree of air trapping, both focal and diffuse. Although this does create issues around increased radiation dose, in certain clinical situations it can be justified, for example the clinician may be suspicious for small airways involvement which is not readily appreciated on the inspiratory HRCT. Expiration can exaggerate these findings by demonstrating mosaic/geographic regions of air trapping. A specific condition where this may be seen is obliterative bronchiolitis.
Strategies should be employed to reduce radiation dose, particularly in the young more vulnerable population. Current new generation CT scanners use iterative reconstruction techniques enabling lower dose scans. Ultra low-dose CT may be considered but keep in mind these ultra low-dose strategies often come at the expense of reduced spatial resolution.
Novel alternatives are emerging including artificial intelligence (AI) powered algorithms. Radiologists can assess the airway to artery diameter ratio (AAR) on CT but the process is time consuming and tends to focus on a limited number of airways rather than the lung as a whole. The integration of AI may replace this manual scoring (measures all AA pairs), improve efficiencies and enable accurate assessment of disease burden involving the whole lung.
HRCT interpretation:
Bronchial dilatation.
This is the most important finding to establish a diagnosis of bronchiectasis. Criteria for the diagnosis are not well defined. No validated radiological criteria for the diagnosis of bronchiectasis exist and many scoring systems exist to quantify severity.
The commonest criterion are airway to artery diameter (AAR), lack of airway tapering and visibility of airways in the periphery of the lung.
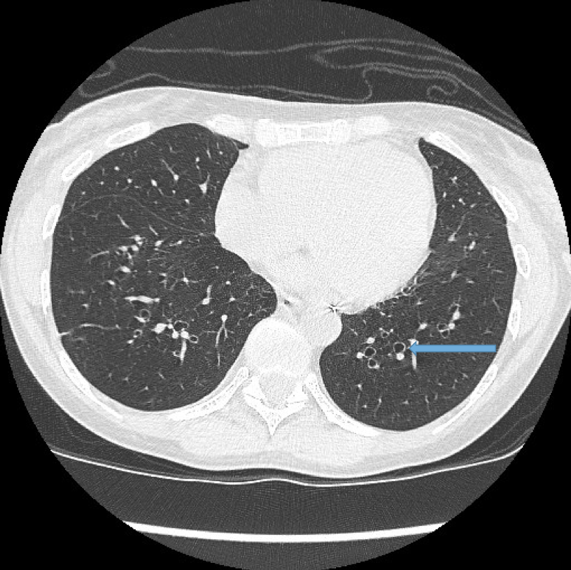
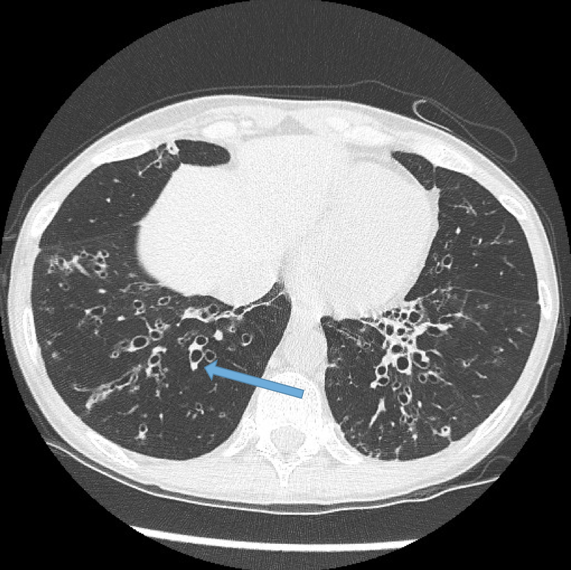
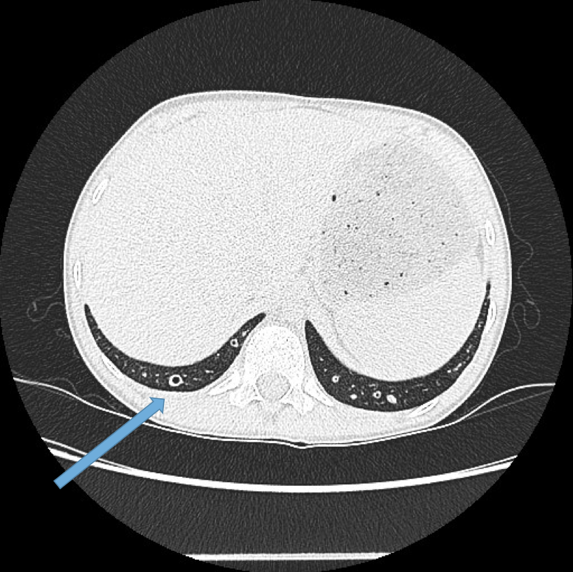
Bronchiectasis is defined as an AAR > 1. This is referred to as the signet-ring sign. Fig 3a, 3b.
There is no consensus on whether to measure the inner diameter vs outer diameter of the airway but inner is more commonly used. Outer diameter is likely more robust as thickened bronchial walls and/or retained mucous reduce the inner diameter on CT resulting in a false negative. Fig 5 and 7.
Airway diameter cut offs also seem to be age-dependent. This ratio increases as we age due to the loss of elastic recoil of the ageing airways. AAR also assumes the pulmonary artery is normal calibre. Local hypoxia (smoking) can reduce pulmonary artery calibre and give a spuriously elevated ratio.
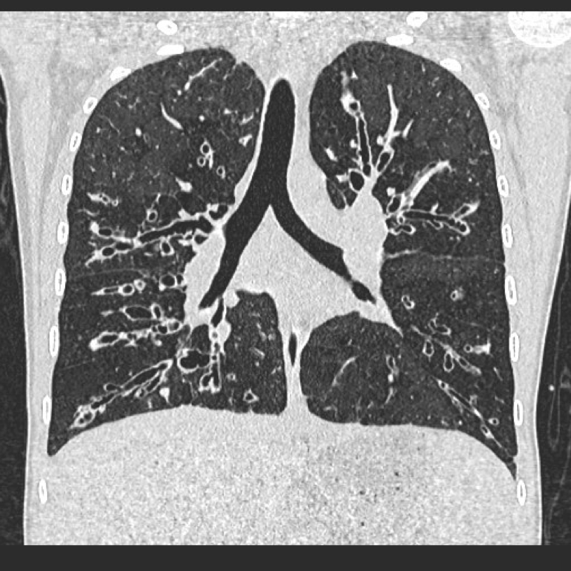
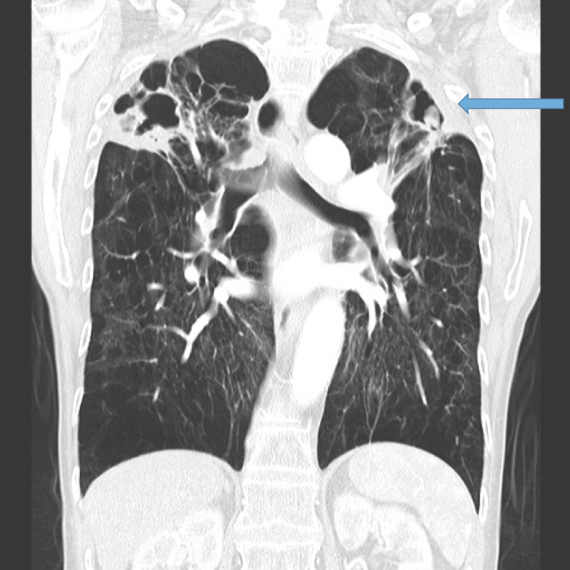
Lack of bronchial tapering.
Normal airways diminish in calibre as they extend toward the lung periphery. Fig 4
Fig 3b. Elderly male patient with COPD and bronchiectasis. Signet ring sign
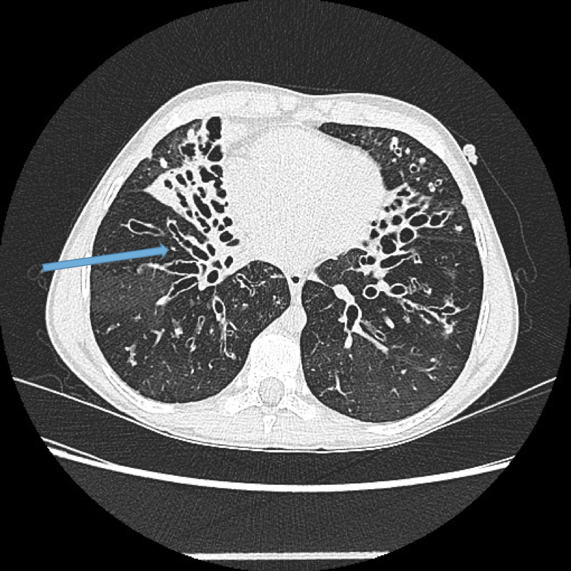
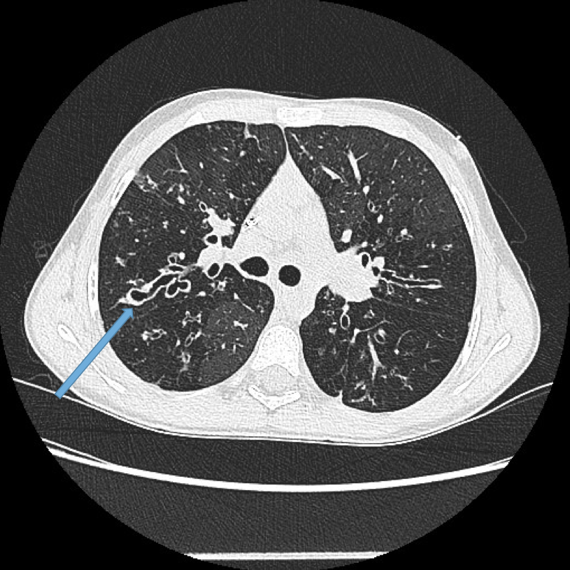
Fig 3c Young adult with cystic fibrosis. Arrow: Cylindrical (tubular) bronchiectasis.
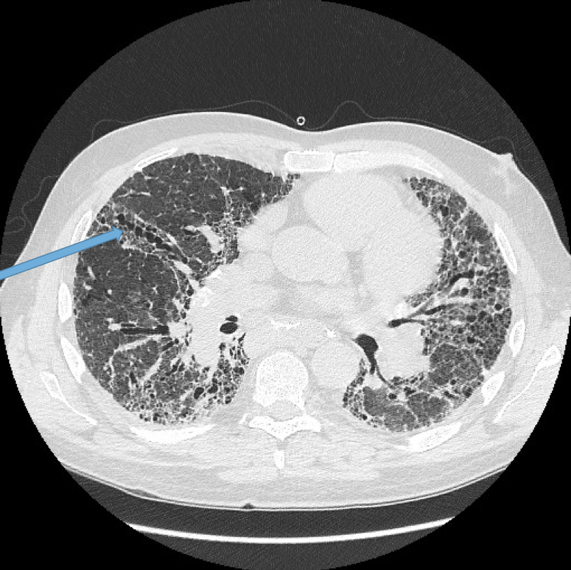
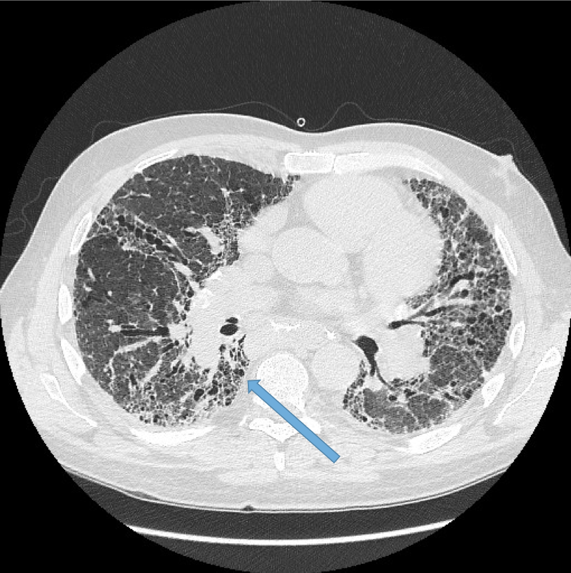
Fig 3d Elderly male with idiopathic pulmonary fibrosis. Arrow: varicose bronchiectasis
Fig 4. Young adult with cystic fibrosis. Coronal CT scan. Widespread bronchiectasis. Lack of bronchial tapering
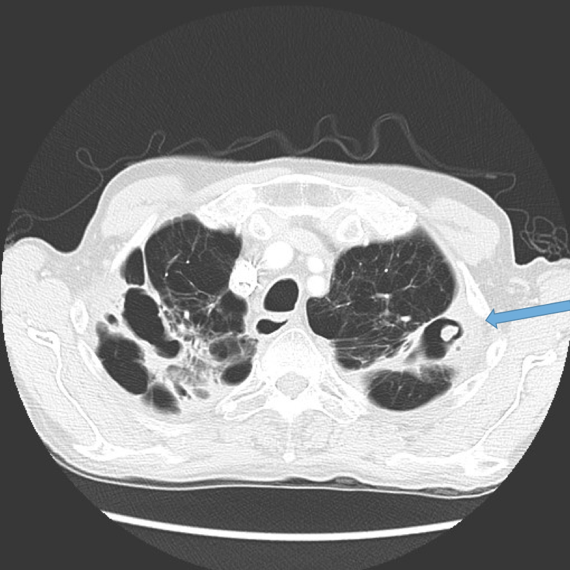
Visualisation of bronchi within 1 cm of the costal pleura or abutting the mediastinal pleural surface Figs 5, 6a, 6b.
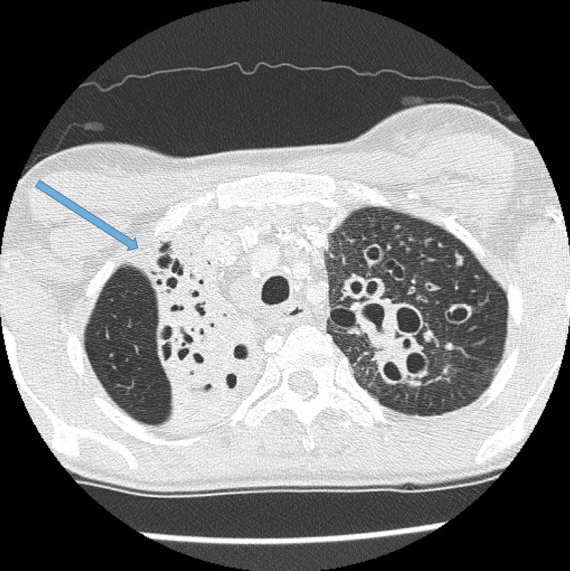
Normal airways should not be visualised this far out in the lung periphery. Fig 5
Mucoid impaction. May be seen as lobular, tubular branching structures. The mucous may become of high density due to chronic inspissation. Fig 7
Bronchial wall thickening. This is non specific and may be reversible if there is an intercurrent infection giving rise to acute bronchitis. Fig 8
Mosaic lung attenuation. This term is used to describe heterogeneous lung density due to air trapping in the affected lung segments and as a result has a geographic distribution. This finding can be produced or exaggerated on expiration. Fig 9, 10a, 10b, 10c.
Fig 5. Bronchi visualised within 1 cm of the costal pleural surface (arrow)
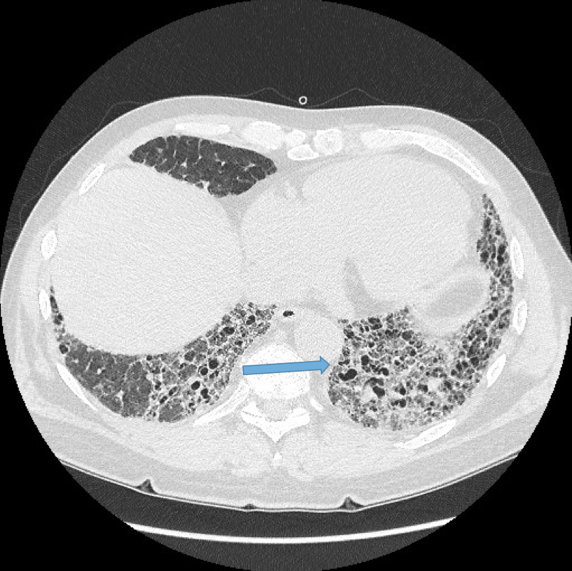
Fig 6a. Elderly male with idiopathic pulmonary fibrosis. Dilated bronchi abutting the mediastinal pleural surface
Fig 6b. Elderly male with idiopathic pulmonary fibrosis. Dilated bronchi abutting the mediastinal pleural surface
Fig 7. Young adult with cystic fibrosis. Mucoid impaction of bronchiectatic airways. This often demonstrates a branching configuration.
Fig 8. Young adult with cystic fibrosis. Marked bronchial wall thickening.
Fig 9. Adult with cystic fibrosis. Mosaic attenuation of the lung due to air trapping in segments of lung affected by bronchiectasis. The air trapping gives rise to hyperlucent (darker) pulmonary segments.
Fig 10a. Adult female with obliterative bronchiolitis secondary to rheumatoid arthritis. Note the mosaic attenuation and bronchial wall thickening but without dilatation.
Fig 10b. Same patient as in a. Severe mosaic attenuation and dilated small airways at the lung bases.
Fig 10c. Marked lung hyperinflation secondary to severe diffuse air trapping in obliterative bronchiolitis.
Vascular abnormalities.
Dilated bronchial arteries. These are best demonstrated post administration of intravenous contrast. These tortuous vessels extend along the central airways toward the hila. It is these vessels that are often responsible for haemoptysis, a symptom these patients may describe. Fig 11
Dilated main pulmonary artery. This usually indicates underlying pulmonary hypertension as a sequelae of chronic, severe lung disease. Fig 12, 13
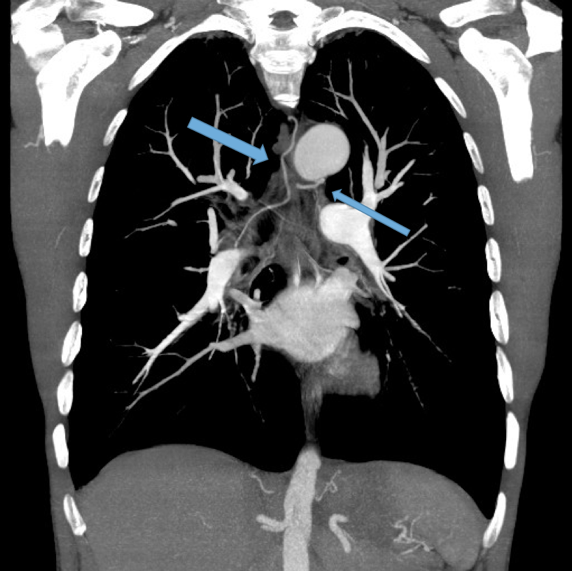
Fig 11. Contrast enhanced CT scan in a coronal reformat. Dilated bronchial arteries course through the mediastinum. (arrows)
Fig 12. Adult female post bilateral lung transplants complicated by obliterative bronchiolitis. Note enlarged central pulmonary arteries (arrows).
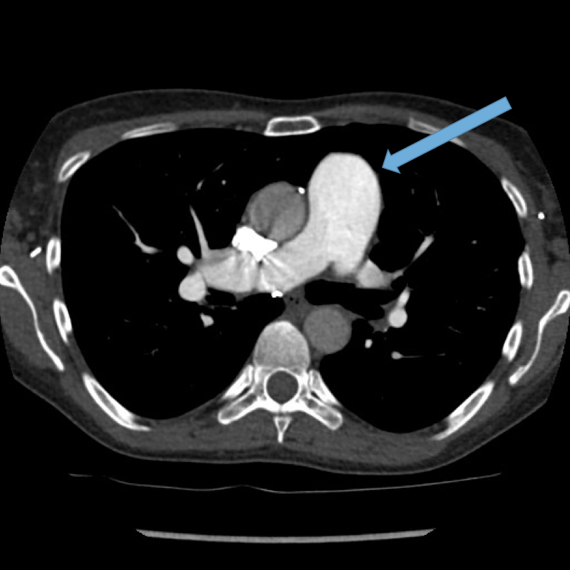
Fig 13. Axial contrast enhanced CT demonstrating enlarged pulmonary trunk in a patient with pulmonary hypertension (arrow).
Other findings
Lobar collapse Fig 14a, b
Mycetoma formation (Fungus ball) Fig 15a, b, c
Aspergillus fumigatus is a fungus that may colonise dilated airways or bullae/cavities. It is an important cause of haemoptysis.
Fig 14a. Young adult with cystic fibrosis. Chronic right upper lobe collapse (arrow)
Fig 14b. Young adult female with cystic fibrosis. Long standing middle and lingular collapse (arrows) Background severe bronchiectasis.
Fig 15a. Elderly male with COPD and upper lobe bronchiectasis and scarring. New haemoptysis. Questionable soft tissue nodule within a left upper lobe bullous (arrow).
Fig 15b. Axial CT scan on lung windows. Mycetoma within the left upper lobe bullous (arrow).
Fig 15c. Coronal reformat demonstrating bilateral upper lobe bullae, scarring and bronchiectasis with a fungus ball on the left (arrow).
CT features predicting mortality (Loebinger et al 2011):
increased wall thickness
emphysema
dilation severity
small and large airway plugging
mosaicism
Conclusion
HRCT continues to be the gold standard for establishing the diagnosis, the anatomic extent and severity of bronchiectasis.
CXR is utilised in the follow up of these patients once a diagnosis has been established, particularly when they present acutely with an exacerbation. As bronchiectasis is a chronic illness often requiring multiple hospital admissions throughout life for acute exacerbations, we must remain cognisant of the cumulative radiation dose to each patient. In difficult to interpret CXR’s or patients who fail to improve post conventional antibiotics, HRCT can be utilised to assist in ongoing management by ruling out unusual infections such as mycetoma, demonstrate new or progressive lobar collapse or to guide bronchoscopy.