Airway clearance in the normal lung
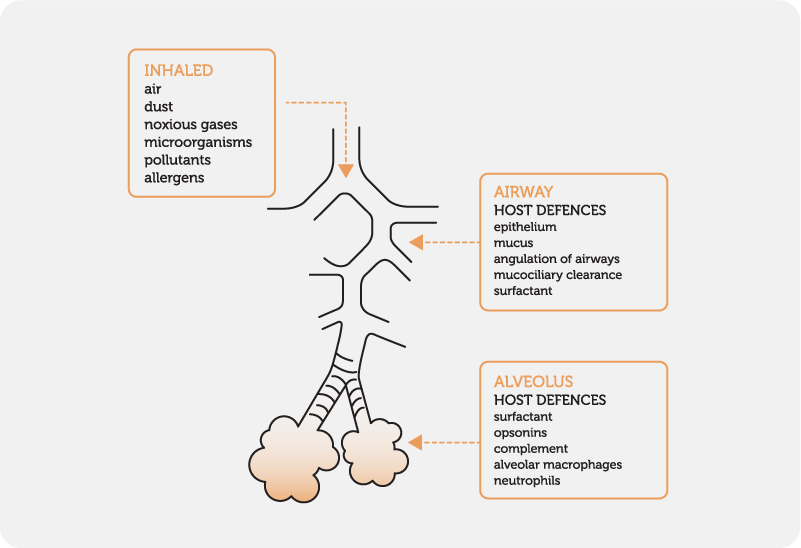
The normal lung is cleared of pollution, dust and foreign particles by several mechanisms (Fig. 1) including :
the mucociliary escalator, also known as mucociliary clearance (MCC)
cough
alveolar macrophages
Mucociliary Escalator
In normal circumstances, approximately 20-30ml of secretions are produced by the airways every day. These secretions, which are necessary to protect the airway from foreign particles, are cleared by the muco-ciliary escalator and swallowed. If the quantity of mucus exceeds this amount, a cough is necessary to clear the airways of the mucus.
The mucociliary escalator covers most of the bronchi, bronchioles and nose. It is composed of two basic parts:
Mucous-producing goblet cells:
Ciliated epithelium:
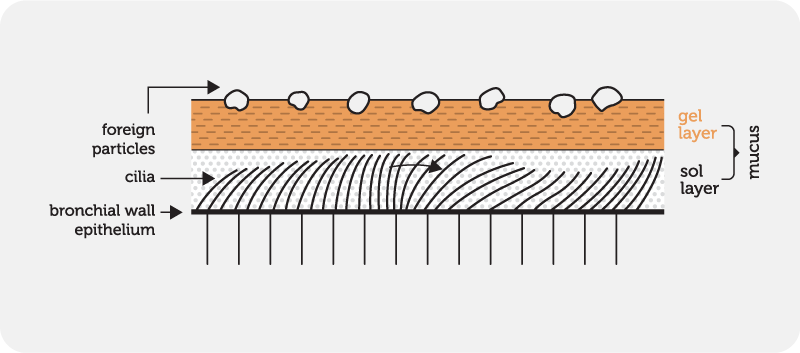
The bronchial wall epithelium is lined with microscopic, hair-like structures called cilia which are surrounded by a thin film of fluid, called the sol layer. These motile cilia have a continual, rhythmic beating motion which pushes secretions from the peripheral to the central airways via the trachea to the throat where they are swallowed or expectorated (hence the term “escalator”).
This layer is less viscous than the gel layer, allowing the cilia to beat freely. During the forward stroke, the tips of the cilia contact the gel layer, thus propelling it downstream, towards the mouth.
This movement of mucus moves at approximately 1mm per minute in peripheral airways, clearing the healthy lung in less than 24 hours.
The mucociliary escalator is a major barrier against infection. In the healthy lung, microorganisms (approximately 100,000 bacteria per day) can be effectively cleared by this mechanism.
If the mucociliary escalator fails, it increases the risk that the normal and potentially pathogenic, inhabitants of the nose, throat and the back of the mouth (nasopharynx), will descend into the lung. The upper airways are home to a diverse microbiota whereas the lower airways, in the healthy lung, are effectively sterile.
Factors inhibiting the mucociliary escalator include:
congenital defects of cilia such as Primary Cilial Dyskinesia (PCD)
cigarette smoke (causes paralysis of the cilia)
dust and pollution
inhalation of toxic gases such as sulphur dioxide (causes paralysis of the cilia)
chronic respiratory diseases such as bronchiectasis where there is damage to the epithelium and the cilia are destroyed
changes in the character of mucus, caused by disease or dehydration
volume of secretions so great that the system is overloaded (bronchiectasis, cystic fibrosis)
low levels of humidity (such as aircraft)
Cough
Cough, which may be initiated either voluntarily or reflexively, is an explosive expiration that provides a normal effective protective mechanism for clearing the tracheobronchial tree of secretions and foreign material, noxious substances and infections from the larynx, trachea and larger bronchi.
To produce a cough, the following sequence occurs:
inspiration
the glottis closes and the vocal cords contract to shut the larynx and trap air within the lungs
the abdominal and internal intercostal muscles contract which significantly raises the intra thoracic pressure
the vocal cords relax and the glottis opens, releasing air at over 160 kph
the rapid air flow clears out any irritants attached to the respiratory lining
Swallowing large amounts of secretions may cause nausea so it is generally recommended to cough into a tissue. This also enables the patient to monitor the colour and quantity of their sputum and to be aware of the presence of any haemoptysis.
Alveolar macrophages
The mucociliary escalator does not extend to the alveoli. Particles deposited in this region are engulfed by macrophages on the surface of the alveoli. The foreign particles engulfed by these macrophages either move up to join the mucociliary escalator or escape via the lymphatic or venous system.
Normal macrophage activity can be impaired by:
cigarette smoke
alcohol
oxidant gases
alveolar hypoxia
radiation
corticosteroids